
International Journal of Environmental and Health Sciences, 1(1), 2018
Author: Benard Wesonga
Affiliation: Dr. Wesonga is a medical doctor currently lecturing at Masinde Muliro University of Science and Technology (MMUST), P.O. Box 190-50100, Kakamega – Kenya
Email Address: bwesonga@adeointl.org
Abstract:
While Home Based Care (HBC) of HIV/AIDS patients is predominantly gaining recognition in most of developing countries in Africa as an alternative approach to Hospital Based Care, its knowledge among the members of local communities in Kenya remains scanty. This study aimed at examining the knowledge of Home Based Care of HIVand AIDS Patients among the people of Butula Division in Kenya. The study was a descriptive study which employed a cross-sectional survey design. The sample included three hundred and seventy seven respondents from Butula Division. Questionnaire method was used to collect data owing to its appropriateness in collecting data from a large sample. A statistical application, namely SPSS aided data analysis process. The study revealed that the majority of the respondents (67.3%) were aware of the existence of Home Based Care of HIV and AIDS Patients in Butula. The major source of their knowledge of HBC was Community Based Organizations. Family and relatives, media, governmental and non-governmental organizations were other sources of their knowledge. The study suggested an initiation of awareness and sensitization programs in the local communities with collaborated efforts from health institutions, government and non-governmental agencies for a sustained knowledge development of HBC of HIV and AIDS patients in rural areas.
Keywords: home based care of HIV and AIDS patients, home based care knowledge, Butula HIV and AIDS home based care, sources of knowledge of home based care, home based care service providers
Introduction
Although in recent years, global commitment to control the HIV/AIDS epidemic has increased drastically, the virus continues to spread with alarming and escalating speed. By the end of 2011 conventional 40 million people living with HIV infection or disease worldwide, approximately 6.2 million in Sub-Saharan Africa were receiving Antiretroviral Therapy(ART), compared to only 100,000 in 2003 (UNAIDS, 2012). The region continues to be the most affected by HIV/AIDS; nevertheless, the virus has rapidly spread to other parts of the world in Asia and parts of Eastern Europe. Various interventions have been put in place in order to address the HII/AIDS menace. Home base care for HIV/AIDS patients has come in handy especially in Africa where health care facilities are not adequate. Traditionally, as DesRosiers, Cupido, Pitout, van Niekerk, Badri, Gwyther and Harding (2014) points out, Home Based Care (HBC) has mainly focused on patients in the terminal stages of HIV/AIDS. However, currently HBC has been extended to include quality of life issues of patients and their families during the course of a life-threatening illness (Simms, Higginson & Harding, 2012).
Globally, in light of decreased HIV/AIDS funding and expanded dependence on HBC all through Africa, a better understanding of how HBC is needed. Best HBC practices can improve patients’ quality of life. In developing countries, many people living with HIV/AIDS are not accepting and receiving the minimum standard of HBC. Of the 5 million individuals living with HIV/AIDS in Sub-Saharan Africa, UNAIDS (2012) estimates that only 250,000 have access to Home Based Care services.
HIV and AIDS discussion has revolved in Kenya for quite a number of years, triggered by the effects experienced both by individuals and communities. Various interventions such as Home Based Care services were advocated as a strategy to ease the growing pressure on hospitals. Home-Based Counselling and Testing (HBCT) can identify HIV infection earlier in the course of the disease progression compared with other testing modalities (Negin, Wariero, Mutuo, Jan & Pronyk, 2009). Nonetheless, the lack of knowledge on HBC identification and engagement in care of individuals with HIV is crucial for the optimization of treatment outcomes and improving results in patients will not be fully comprehended unless diagnosed patients engage with care in a timely manner. In the face of a growing scourge of historic magnitude, the procurement of exhaustive palliative care signifies a critical, but neglected, global priority (Wachira, Kimaiyo, Ndege, Mamlin & Braitstein, 2012). Thus, knowledge of HBC remains fundamental especially in developing economies.
This study investigated the Knowledge of Home Based Care of HIV/AIDS Patients in Butula Division, Busia Subcounty in Kenya. The rationale of study was informed not only by HIV and AIDS Patients’ lack of adequate knowledge on Home Based Care services but also by the lack of empirical evidence on knowledge about Home Based Care Services among HIV/AIDS Patients in Butula Division, Kenya.
Materials and Methods
The study employed descriptive cross-sectional survey research design. The design was appropriate since it allows data collection from a sample which is statistically representative (Owens, 2002) and makes use of various data collection methods including questionnaire, interviews methods. Further, the design allows use of quantitative approach in analysis. The target population included members of local communities in Butula Division. Cluster and random sampling procedure were used to arrive at three hundred and seventy seven respondents from the division. The division was first clustered into its locations from which a list of households was prepared. A representative number of respondents were picked from the list using simple random sampling procure. Data were collected using questionnaire method. The choice of this method was informed by the following reasons: administration is comparatively inexpensive and easy even when gathering data from large numbers of people spread over wide geographic area, reduces chance of the researcher’s bias because the same questions are asked of all respondents and is easy to code and tabulate data. Descriptive statistics were used to report the findings. A statistical application, namely IBM SPSS aided data processing. The processed data were reported using frequencies and percentages and summarized using Tables and Figures.
Results
Demographic Characteristics of the Respondents
The demographic characteristics of the respondents included sex and age. Out of the three hundred and ninety three respondents who took part in the study, 31.8% of them were male. The remaining 68.2% were female. The age distributions showed that majority of them, (62%) were between the ages of 21 to 25 years. The mean age bracket was between 30 to 39 years.
Knowledge About the Existence of Home Based Care Services
The study sought to establish about the existence of knowledge Home Based Care services among the people of Butula Division in Busia. They were asked to indicate whether they had heard about home based care of HIV and AIDS patients and the sources of their knowledge of the services.
Whether ever heard about Home Based Care. When asked about whether they had ever heard about home based care of HIV/AIDS patients, slightly over two third of the respondents, (67.3%) confirmed that they had heard about the services. However, almost a third of them, (32.7%) indicated that had not heard about the services.
Sources of knowledge. The community members have various sources of getting information. In order to establish the source of community’s knowledge of HBC of HIV and AIDS patients, the respondents were asked to identify the source of information about HIV and AIDS patients in Butula. Figure 1 presents their responses.
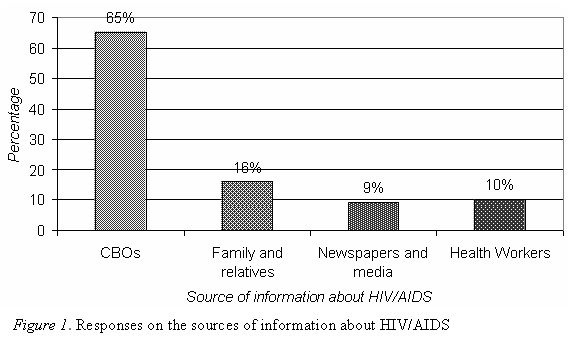
As shown by Figure 1, almost two third (65%) of the respondents indicated that Community Based Organizations were the main sources of their knowledge of HBC of HIV and AIDS patients in Butula. Another 16% of them indicated that family and relatives were also a source of their knowledge. This was followed by 10% who indicated that their source of knowledge was health workers from the Government, NGOs and Churches. Newspapers and media was the least source of knowledge with only 9% of the respondents.
The Institutions Providing Home Based Care in Butula Division
The study also sought to find out whether the respondents knew which institutions provided home based care in Butula Division. The respondents were provided with a variety of home based care service providers which they were required to choose from. Their responses are shown in Table 1.
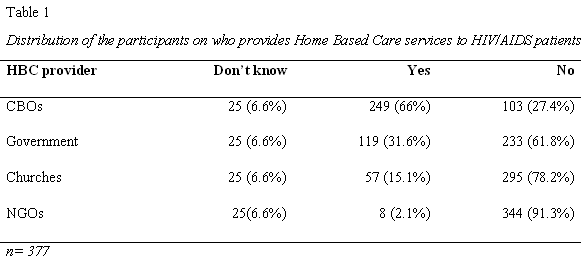
A two third, (66%) of the respondents identified the major providers of Home Based Care services as Community Based Organizations. Almost a third (31.6%) indicated that Government was another key provider. Another 15.1% of them indicated that churches provided home based care. Only 2.1% of them indicated that International NGOs did provide home-based care in Butula.
Discussion
The findings of the study showed that majority of respondents, (67.3%) acknowledged that they were aware of the existence of Home Based Care of HIV and AIDS patients in the community. However, an earlier study conducted by Malale (2011) had found that there was low knowledge of Home Based Care among family care givers for Persons Living with HIV/AIDS (PLWHA). This could be attributed to lack of adequate sensitization campaigns from HBC providers. High knowledge about HBC of HIV/AIDS patients in this study could be linked to the work of CBOs working with the community members in the division. Despite this level of awareness, there was a considerable number of the respondents, (32.7%) who felt that they lacked adequate knowledge of HBC, a pointer that much more needed to be done.
According to a study conducted by WHO (2002) in Thailand, Haiti, Cambodia, Botswana and Kenya on Community Home-Based Care, between 70 percent and 90 percent of illness care takes place within the home and that most PLWHA preferred to be cared for at home. However, the report further states that some HIV and AIDS clients and family members who require HBC may not be aware of the services and how to access home care. WHO (2010) further reported that health and social welfare staff working in hospitals and clinics sometimes are not aware of HBC programs. As a result, HBC is missing in the hospital discharge plan thus affecting continuity of follow up care at home by care givers. These findings show that there is a general of lack of knowledge of HBC services leading to non utilization of the services by PLWHA.
According to 66% of the respondents, the major providers of HBC of HVI/AIDS in Butula were Community Based Organizations; another 31.6% of them indicated that Government also a key provider. Only 2.1% of them indicated that International NGOs did provide Home-Based Care. A study by Kaluba (2011) however had shown that NGOs, Faith Based Organizations (FBO) and government do initiate a number of HBC programs.
The main source of information and knowledge about HBC services according to the study was Community Based Organizations (65%), family and relatives (16%), health workers (10%) and newspapers and media (9%). These findings are consistent but lower when compared to the findings contained in National Committee for AIDS, Drug and Prostitution Prevention and Control (2011) report. The report indicated that the main sources of information included: television/radio/magazines, posters, meetings, leaflets and books, health professionals, teachers and schools, friends and family. The report also showed that urban young people appear to be at an advantage in having many sources to access HIV information (57.5%) compared with their rural counterparts (46.7%). The family was the second most commonly reported source of information (88.2%). Higher percentages of rural young people (82.9%) had accessed HIV information from professional services. In contrast, the media (9%) and family and relatives (16%) in the current study were not the major source of information. This could be attributed to low media penetration in rural areas of Kenya. Further, there could be low or total lack of media coverage of programs related to HBC of HIV/AIDS patients in rural areas. Families are also not likely to talk much about HIV/AIDS patients because of the trauma associated with it.
Conclusions and Recommendations
Conclusions
The main source of knowledge of Home Based Care of HIV/AIDS patients in Butula came from CBOs whose funding is erratic. Thus, the high knowledge gained through CBOs route may not be sustainable without effective support from the relevant health care providers.
Family and relatives contributed little as a source of knowledge. This may be associated with cultural taboos and myths, coupled with misconceptions and stigmatization around HIV/AIDS.
Recommendations
Health institutions are to come up with awareness and sensitization programs that support home based care through Community Based Organizations. This would require additional resources to all health institutions to support home based care services in collaboration with CBOs that provide these services for sustainability.
Community Home Based Care initiatives by the Government should be well collaborated to strengthen the use of multiple channels for knowledge acquisition to effectively educate the communities on home based care as part of the national health care goals.
All stakeholders in the health care need to be fully involved in collaborating with and strengthening community health workers so as to support the national and international health care goals towards caring for the sick at home. Linkages should be created between CBOs and health care providers to ensure the sustainability of the HBC services.
Since there are associated society based perceptions of HIV/AIDS patients, there is need to create awareness about the commonly held cultural taboos among health providers at community level.
The findings in a broader-spectrum have inference in regards to influencing effective strategic health care plan in guiding the implementation of home based care in developing nations.
References
DesRosiers, T., Cupido, C., Pitout, E., van Niekerk, L., Badri, M., Gwyther, L., & Harding, R. (2014). A hospital-based palliative care service for patients with advanced organ failure in Sub-Saharan Africa reduces admissions and increases home death rates. Journal of Pain and Symptom Management, 47(4), 786-792
Kaluba, D. (2011). Factors affecting utilization of community home based care services by people living with HIV/AIDS in Chongwe District, Zambia (Master’s thesis). Retrieved from http://dspace.unza.zm:8080/xmlui/handle/123456789/806
Malale, K. I. J. A. (2011). Home based care for people living with HIV/AIDS: Assessment of knowledge, attitude and practice among family care givers at Ukonga ward in Ilala District. Dar Es Salaam Medical Students’ Journal, 18(1), 23-31
National Aids Control Council. (2000). Kenya national HIV/AIDS strategic plan. Nairobi: National Aids Control Council
Negin, J., Wariero, J., Mutuo, P., Jan, S., & Pronyk, P. (2009). Feasibility, acceptability and cost of home-based HIV testing in rural Kenya. Tropical Medicine and International Health, 14(8), 1–7. doi:10.1111/j.1365-3156.2009.02304.x
Owens, L.K (2002). Introduction to survey research design. Retrieved from http://www.srl.uic.edu/seminars/ Intro/introsrm.pdf
Simms, V., Higginson, I. J., & Harding, R. (2012). Integration of palliative care throughout HIV disease. The Lancet Infectious Diseases, 12(7), 571-575
The National Committee for AIDS, Drug and Prostitution Prevention and Control. (2011). National Strategy on HIV/AIDS Prevention and Control in Viet Nam up to 2010 with a vision to 2020
UNAIDS. (2012). Together we will end AIDS. Geneva: UNAIDS
Wachira, J., Kimaiyo, S., Ndege, S., Mamlin, J., & Braitstein, P. (2012). What is the impact of home-based HIV counseling and testing on the clinical status of newly enrolled adults in a large HIV care program in Western Kenya?. Clin Infect Dis. 54, 275–281
World Health Organization. (2002). Community health based care in resource limited settings; A framework for action. Retrieved from http://www.who.int/hiv/pub/prev_care/isbn9241562137.pdf
World Health Organization. (2010). Community involvement in care and support. Retrieved from http://www.afro.who.int/index.php?option=com_content.&view=article&id=2234
Citation
Wesonga, B. (2015). Knowledge of home based care of HIV and AIDS patients in Butula division, Kenya. International Journal of Environmental and Health Sciences, 1(1). Retrieved from http://writersbureau.net/journals/ijehs/knowledge-of-home-based-care-of-hiv-and-aids-patients-in-butula-division-kenya.pdf
ACCESS > Printer-friendly Version